Contraceptive Use and Unintended Pregnancy
Authors
INTRODUCTION
At any one time, most women of reproductive age in the United States would like to avoid becoming pregnant. Half of all 15–19 year old adolescent girls in the United States have had intercourse; the others begin soon after, so that only 3% of all women aged 25–29 years have never had intercourse (Table 1). Yet, the most frequently desired number of children is two, leaving most of a woman's years between “sexual debut” and menopause ones in which neither they nor their partners wish to become pregnant.
Table 1. Percentage distribution of women ages 15–45 according to exposure to the risk of unintended pregnancy by age and union status (National Survey of Family Growth, 2002)*
Eleven percent (6.7 million) of all women in the United States aged 15–44 years are not at risk of unintended pregnancy because they have never had sexual intercourse, and another 7% (4.4 million) are not currently in a sexual relationship. An additional 3% (1.9 million) are sterile for reasons other than contraception. This includes both those who have passed menopause and those who cannot conceive as a result of physical or surgical sterility of themselves or their partner. Finally, 9% (5.8 million) of women are not at risk for unintended pregnancy because they either are currently pregnant, recently had a baby, or are trying to become pregnant.1, 2
The proportion of women who are at risk of unintended pregnancy varies across age groups (see Table 1). Among adolescent girls aged 15–19 years, only 38% are at risk, primarily because a large proportion (56%) are not having intercourse. The proportion not currently having sexual intercourse drops to 18% of 20–24 year-olds and to 8–11% of women aged 25 years and older. Among women 20 years and older, 69–79% are at risk of unintended pregnancy, depending on age group. The proportions of women who are pregnant or trying to become pregnant are greatest from age 25–34 years (14%), whereas the percentage of women who are noncontraceptively sterile is quite low (1–3%) for all women under age 40, and then jumps to 9% for women aged 40–44 years.
The proportion of women at risk is highest for those who are currently married (79%) or cohabiting (81%), but sex and marriage are not so closely linked as they were 20–30 years ago. Between the typical age of first intercourse for women and the typical age of marriage, there is a 7 year gap for young women and a 10 year gap for young men in the United States. This time period is widening as young people become sexually active at increasingly younger ages and marry at older ages.3 Half (52%) of all never-married, noncohabiting women aged 15–44 years are at risk of unintended pregnancy. Just as it cannot be assumed that a woman who is having intercourse is married, neither can it be assumed that once married, always married. One in five women aged 15–44 years who have ever been married is separated, divorced, or widowed. Most of these women are in a sexual relationship, however, and three quarters (73%) are at risk of unintended pregnancy. Among the 42.7 million women aged 15–44 years who are at risk of unintended pregnancy, 47% (20.3 million) are not currently married.1
AVAILABILITY OF CONTRACEPTIVE METHODS IN THE UNITED STATES
A variety of contraceptive methods is available to women and men in the United States. The most effective methods must be obtained by prescription or insertion by a clinician. These include oral contraceptives (OCs), long-acting hormonal methods (the injectable, the implant, the patch and the vaginal ring), intrauterine devices (IUDs), diaphragms, and cervical caps. In addition, surgical contraceptive sterilization is available to both men and women. Condoms (male and female) and spermicides, such as foams, jellies, and suppositories, are available without prescription. Instruction in the various methods of ovulation prediction and periodic abstinence is available from nonmedical sources as well as physicians and nurse clinicians. Use of certain OCs as emergency contraception has been approved by the US Food and Drug Administration (FDA), and these are currently available either by prescription or, for women aged 18 and over, emergency contraception can now be obtained directly from pharmacies (behind the counter).
CONTRACEPTIVE SERVICE PROVIDERS
In the United States, women receive contraceptive services from private practice general and family practitioners and obstetrician-gynecologists, as well as from publicly supported clinics run by hospitals, health departments, Community Health Centers, and Planned Parenthood affiliates or independent clinic providers. In addition, some teenage and young adult women receive contraceptive services from school-based clinics and college or university health centers.
Approximately three in four women obtaining contraceptive or other reproductive health services in the past year report going to a private practitioner or Health Maintenance Organization for their care; one in five visits a publicly funded clinic; and 4% are served in hospital emergency rooms, urgent care centers and by other types of providers.4 Among those seeking care from private providers, two-thirds receive that care from obstetrician-gynecologists, 21% from family physicians, 11% from internists and 2% from other provider types.5
Among all women receiving any sexual or reproductive health care service over the course of one year, 57% receive a contraceptive method or a check-up related to method use, 90% receive preventative gynecological care such as a pap test or pelvic exam, 30% receive pregnancy-related care (pregnancy test, prenatal care, abortion) and 31% receive STD testing or treatment or HIV testing.4
The most common expected source of payment for women's visits involving sexual and reproductive care is private insurance (67%). One in ten women pay for the visit themselves, 12% receive care paid for by Medicaid, 9% from other government programs or sliding fees, and 2% from other sources. Payment source varies tremendously according to type of provider. Eighty percent of women getting SRH care from private physicians rely on private insurance to pay for their care; in comparison only 19% of women served by publicly funded clinics use private insurance to pay for their care.6
Annually, some seven million US women receive contraceptive services, supplies, and information from nearly 8,000 publicly supported family planning clinics, located in 85% of all US counties. The largest proportion (37%) of clinics are run by public health departments, and these serve 33% of all clinic clients. Planned Parenthood clinics also account for 33% of all clients, whereas hospital family planning clinics serve 10%, and community and migrant health centers serve 10%. Clinics run by independent agencies such as community action groups, neighborhood health centers, and women's health centers account for 13% of all contraceptive clients.7
Family planning clinics, using a combination of federal, state, and local funds, provide care to those who cannot afford services from private physicians or who cannot use private physicians for other reasons. In most clinics, fees are based on the client's ability to pay, confidential services to teens are assured, and a range of contraceptive methods is offered. As a result, family planning clinic clients are primarily low-income (40% are below 100% of the federal poverty level and 35% are between 100% and 249% of the federal poverty level), and young (22% are younger than age 20 years, 42% are aged 20–29 years). And, the majority of clinic clients are from ethnic or racial minority groups (21% are black, 28% are Hispanic, and 7% are Asian or other races).6 Lower income women go to clinics primarily because they cannot afford physicians' fees, because the clinic is more conveniently located, or because the clinic accepts Medicaid payment. Adolescents often go to clinics because of the free or low-cost services and because they are afraid a private physician will tell their parents about their contraceptive use. In addition, some women, especially teenagers who have never been to a physician on their own, go to clinics because they do not know a physician who would serve them. Clinic clients usually shift to private physicians when their incomes rise and as they become older.
Fifty-eight percent of all publicly supported clinics receive federal Title X support and must therefore follow federal standard-of-care guidelines. These guidelines provide both medical protocols as well as mandates regarding confidentiality and key areas of outreach that clinics should seek to address. As a result, many publicly supported clinics provide outreach and information or education in local schools or in other community locations. These clinics often seek to reach out to women (and men) in need of contraceptive care who have special needs or risk factors for unintended pregnancy (e.g. because of homelessness, drug or alcohol abuse, or domestic violence).
The provision of contraceptive services, like all areas of healthcare, has been affected by changes in the structure of healthcare financing and the rise of managed care. In the past, most privately insured women had employer-based indemnity health insurance plans that rarely covered either routine gynecologic checkups or reversible contraceptive services and supplies. However, such plans often covered sterilization services. Today, most privately insured women are enrolled in managed care plans. These plans are more likely to cover preventative care, including routine gynecologic checkups and some reversible contraceptive services and supplies. However, not all managed care plans cover all or even most methods, and often the process of obtaining contraceptive services within managed care plans places additional burdens on women seeking contraceptive care. These burdens include prior authorization requirements that may cause some women to delay care or forgo sensitive care that a woman may not want to disclose to her primary care physician.8
ATTITUDES ABOUT CONTRACEPTIVE METHODS
Women and men in the United States often have inaccurate fears about the risks of contraceptive methods, especially OCs, other hormonal methods, and IUDS, and they often judge the available methods unfavorably. The percentage of women reporting a favorable opinion about specific methods is highest for OCs, the male condom, vasectomy, and tubal ligation. Except for OCs, which 78% view favorably, no more than two thirds feel favorably about any other method. In fact, only 26% have a favorable opinion of the diaphragm, and fewer feel positively about implants, injectables, spermicides, the IUD, the female condom, or the cervical cap. Opinion about methods recently introduced into the United States (implants, injectables, and the female condom) may change as more women become aware of them.9
Whereas many women worry about the side effects of available methods, often they are not aware of a method's health benefits, such as OCs reducing the risk of ovarian cancer. Although concerns about OCs center on fears of side effects and health risks, the method usually receives favorable ratings on effectiveness, lack of interference with intercourse, and convenience. In contrast, those who judge condom, diaphragm, and spermicides unfavorable generally do so because of concerns about effectiveness, interference with intercourse, and the inconvenience these methods entail. Growing awareness of the risks of sexually transmitted diseases, including human immunodeficiency virus (HIV) infection and acquired immunodeficiency syndrome (AIDS), has resulted in increasingly favorable attitudes about latex condoms, which are the one method that has been shown to decrease the risk of HIV infection and AIDS. The chief concern about periodic abstinence and withdrawal methods is their effectiveness.
PATTERNS OF CONTRACEPTIVE USE
Among all women aged 15–44 who are at risk of unintended pregnancy, approximately nine in 10 are currently using a contraceptive method (Table 2). Thirty-two percent rely on contraceptive sterilization of themselves or their partner, just over half (52%) use reversible medical methods, 5% use nonmedical methods such as withdrawal and periodic abstinence, and 11% use no contraceptive method, even though they are at risk of unintended pregnancy.1
Table 2. Percentage distribution of women at risk of unintended pregnancy by contraceptive method use and age, union status, race/ethnicity, and poverty (National Survey of Family Growth, 2002)*
(Numbers do not all total 100 because of rounding.)
Patterns of contraceptive use differ by age. The proportion using reversible medical methods declines steeply with age from more than four of five women ages 20–24 years to fewer than one quarter of those ages 40–44. OCs are the most commonly used method among women younger than 30 years of age, accounting for 34–46% of these women. Condoms are second in popularity among this age group, accounting for 18–22% of women in this group. Although only 5% of all women at risk use injectable contraceptives, this method has grown in popularity since its introduction in the United States, particularly among young women. Twelve percent of teens at risk used this method. As women become older and complete their families, male and female contraceptive sterilization becomes increasingly common, rising steeply from 4% of women at risk ages 20–24 to nearly one in five women in their late 20s and to nearly two of three women ages 40–44.
The proportion of women at risk of unintended pregnancy who use no contraceptive method is highest among never-married women, 16% compared to 8% of those who are currently married and 10–11% of cohabiting or formerly married women. Sterilization is the most frequently used method among women who are currently married (42%) as well as formerly married women (52%). The pill is the most commonly used method among never-married women (41%) and cohabiting women (30%). Condoms are most likely to be used by never-married women (20%).
The growing awareness of the protection that latex condoms give against contracting sexually transmitted diseases, including AIDS, contributed to an increase in condom use among never-married women using contraception from 12% in 1982, to 15% in 1988, to 30% in 1995. But, between 1995 and 2002, condom use declined among never-married women to 20% (although some women do use condoms along with other hormonal methods, and this is not accounted for in Table 2). 1, 10
Although poor women and minority women at risk of unintended pregnancy have, in the past, been more likely than higher income and non-Hispanic white women to be using no contraceptive method, these differences lessened during the 1980s and 1990s. Between 1982 and 1995, the percentages of women at risk using no method declined so that in 1995 there were no significant race/ethnicity or poverty differences (Fig. 1). However, by 2002, these gains had reversed themselves and disparities in nonuse were again evident.11 In addition, there is some variation in the types of methods used according to these income and race/ethnicity subgroups. Low-income women are less likely to rely on reversible methods and more likely to rely on sterilization than higher income women. Thirty-seven percent of women at risk of unintended pregnancy who are below 100% of the poverty level use sterilization compared to 30% of women at 250% of poverty and above. Poor women relying on sterilization are more likely than higher income women to have been sterilized themselves rather than have a partner who has a vasectomy.
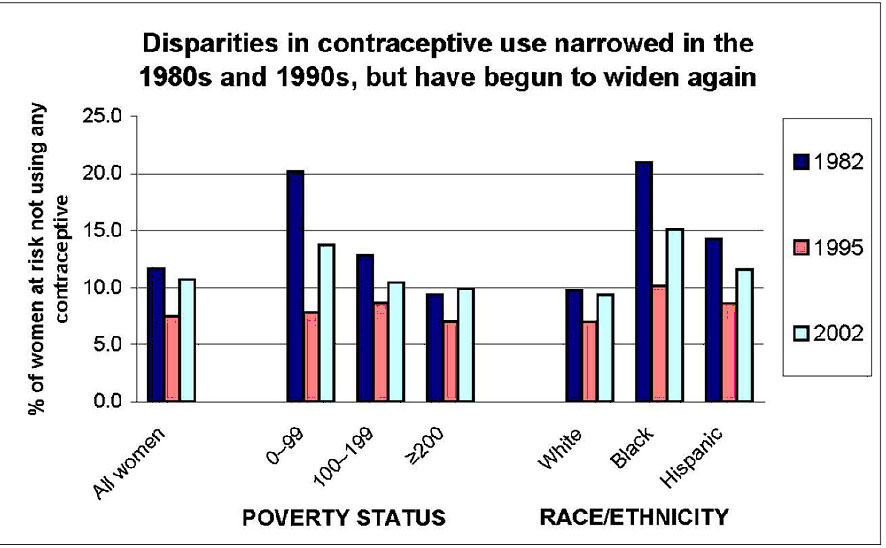
Fig. 1. Disparities in contraceptive use narrowed in the 1980s and 1990s, but have begun to widen again. Source: Guttmacher Institute, 2008, special tabulations of the 1982, 1995 and 2002 National Surveys of Family Growth
NONUSERS OF CONTRACEPTION
Over the course of one year, many women experience periods when they do not use contraception, even though they are at risk for unintended pregnancy. Among non-sterilized adult women (aged 18–44) at risk for unintended pregnancy, nearly one in four (more than six million women) experience a gap in contraceptive use of one or more months: 8% use no method for all 12 months and 15% have a gap of one month or longer.12, 13
Many women with periods of nonuse report difficulties using or accessing methods; others cite infrequent sexual activity, ambivalence about becoming pregnant, and misperceptions about pregnancy risk. In addition, for more than half of women who have a gap of at least one month, the period of nonuse coincides with an important life event, such as the beginning or ending of a relationship, a move to a new home, a job change, or a personal crisis.
Some women have more difficulty than others with continuous method use. For example, disadvantaged women and women who are more ambivalent about avoiding pregnancy are more likely to have had a gap in method use. Women who have little education, who belong to minority groups or who are poor have a relatively high likelihood of having a gap in use of at least one month, as do those who are covered by Medicaid.12, 14
Although 62% of women who are risk for unintended pregnancy report that it is very important to avoid a pregnancy, 20% say it is only somewhat important, and 18% say it is of little or no importance. Almost four in ten women who said avoiding pregnancy was of little or no importance reported having had a gap in contraceptive method use of at least one month, compared with fewer than two in 10 of those who said avoiding pregnancy was very important.12
Among low-income women at risk of unintended pregnancy, method use is more common among those who have been to college, cohabiting and never-married women, those in a relationship for a year or more, women with one to two children, and those wanting to have children in the future. It is less likely among those who would be glad if they became pregnant and among English-speaking Hispanic women. Women at risk are more likely to use a contraceptive if they are satisfied with the care they receive from their gynecologic provider, if they talk frequently with their partner or girlfriends about contraception, if they feel strongly that they do not need their partner's approval for contraceptive use, if they believe contraception is important in preventing pregnancy, and if they think that their friends see contraceptive use as important.15
UNINTENDED PREGNANCY
Half of all pregnancies (49%) in the United States are unintended.16, 17 Hence, they occur to women who want to have a baby later but not now (generally called mistimed) or to women who did not want to have any (more) children at all (called unwanted) (Table 3). The proportion of pregnancies that are unintended is highest among adolescents (82%) and varies considerably by age. The percentage of pregnancies that are unintended is lowest among women aged 30–34 years (33%) and rises again among older women to 38% among women 40 years of age and older. Unintended pregnancies are also relatively more likely to occur among never-married women (77%), black women (69%), and low-income women (62% for women below 100% of the federal poverty level).
Table 3. Percentage of all pregnancies (excluding miscarriages) that are unintended by women's age, marital status, race, ethnicity and poverty status (1987, 1994 and 2001)
Women's characteristics | Percentage of all pregnancies that are unintended | ||
1987* | 1994† | 2001‡ | |
All women | 57% | 48% | 49% |
Age | |||
15–19 | 82% | 77% | 82% |
20–24 | 61% | 57% | 60% |
25–29 | 45% | 39% | 43% |
30–34 | 42% | 32% | 33% |
35–39 | 56% | 38% | 29% |
40–44 | 77% | 45% | 38% |
Marital status | |||
Currently married | 40% | 28% | 27% |
Formerly married | 69% | 68% | 63% |
Never married | 88% | 76% | 77% |
Race | |||
White | NA | 42% | 40% |
Black | NA | 69% | 69% |
Hispanic | NA | 48% | 54% |
Poverty status | |||
<100% poverty | 75% | 61% | 62% |
100–199% | 64% | 53% | 57% |
200+% poverty | 45% | 39% | 38% |
NA = not available.
*Forrest JD: Epidemiology of unintended pregnancy and contraceptive use. Am J Obstet Gynecol 170:1485, 1994
† Henshaw SK: Unintended pregnancy in the United States. Fam Plann Perspect 30:24, 1998
‡Finer LB and Henshaw SK: Disparities in rates of unintended pregnancy in the United States. Persp Sex and Reprod Health 38:90, 2006
The percentage of pregnancies that are unintended has declined in recent years from 57% in 1987 to 48% in 1994 and remained stable between 1994 and 2001 (see Table 3). These declines have occurred across all age categories but have been more significant among older women. They have also been more significant among low-income women. In 1987, 75% of all pregnancies to women with family incomes below 100% of the poverty level were unintended. This dropped to 61% in 1994 and 62% in 2001. In comparison, the percentage of unintended pregnancies to women with incomes at 200% or more of the federal poverty level fell from 45% in 1987 to 39% in 1994 and 38% in 2001.
Among all unintended pregnancies, about half (48%) end in an abortion whereas 52% result in an unintended birth. This relationship differs for adolescents, who are more likely to resolve unintended pregnancies with a birth. Sixty percent of all unintended pregnancies to adolescents result in an unintended birth, whereas 40% are resolved with an abortion. These percentages represent a significant change in the resolution of unintended pregnancies among adolescents. Throughout the 1980s, adolescents who were pregnant unintentionally were more likely to obtain an abortion (53–55%) than to carry the pregnancy to term.
Forty percent of all women aged 15–44 have had at least one unintended pregnancy at some time in their lives; 31% have had one or more unplanned births. Given current rates of pregnancy and abortion, by the time they are 45 years old, more than half of all women in the United States will have experienced an unintended pregnancy and 35% will have had an abortion.18
The level of unintended pregnancy in the United States is high compared with most other industrialized countries.19 The difference is especially striking among adolescents, although unintended pregnancy and abortion rates also are high among adult women in the United States. Although there is no evidence that the young women in the United States are more (or less) sexually active than the young women in many other industrialized countries, the United States has adolescent pregnancy rates that are six to seven times higher than the rates for the Netherlands, three to four times higher than the rates for Sweden and France, and nearly twice as high as the rates for Canada and for England and Wales (Fig. 2). The factors responsible for these differences are not entirely clear; however, it is likely that they are due, in part, to differences in the levels of disadvantage among countries, to variation in the family planning education and services provided to youth, and to greater or lesser openness regarding sexuality among countries.
|
The high levels of unintended pregnancy and abortion in the United States result from two basic factors. The primary factor is that many women at risk of unintended pregnancy do not use any contraceptive method, usually because of gaps between methods or between stable relationships. The secondary factor is the relatively high rates of ineffective use among those who are using contraceptive methods. Although technologic improvements in contraceptive methods can reduce both these factors, the greatest impact comes from stronger motivation by women and men to avoid unintended pregnancy and from increased awareness of the comparative benefits and risks of methods and of nonuse, and knowledge on how to use contraceptives effectively.
FAMILY PLANNING INFORMATION AND EDUCATION
There is rising public concern over the occurrence of unintended pregnancy and, particularly, of unintended, nonmarital adolescent pregnancy and childbearing in the United States. This has drawn attention to the manner in which young people are educated about sexuality, contraception, and how to avoid pregnancy and other negative consequences of sexual activity. Parents and other adults have long played a key role in controlling the sexual behavior of adolescents and in providing basic information about sex and pregnancy avoidance. During the past 25 years, there has been a proliferation of organized efforts to augment the information, education, and support traditionally provided by families. Beginning with programs and services for young, pregnant women, these efforts have expanded to include legislative mandates regarding the teaching of sexuality or family life education in schools, development and distribution of a variety of sexuality education curricula, as well as integrated community interventions and media involvement. Organized efforts to implement sexuality education and related activities have also been influenced by growing public concern and awareness of HIV/AIDS and the need to provide young people with the information and means to avoid infection.
Increasingly, policies and programs to encourage abstinence among unmarried teenagers have become popular. Some of these programs attempt to accomplish this objective by giving young people encouragement, offering moral support, and teaching interpersonal skills to resist pressures to become sexually active. Others seek to convince teenagers that sex before marriage is immoral, and emphasis is placed on the negative consequences of sexual intercourse while occasionally withholding or distorting information about the availability and effectiveness of contraception.20 In fact, although most public schools provide some sort of sexuality education to middle or junior and senior high school students, the education provided is often too little, too late.
On a broader scale, community and service organizations have implemented interventions aimed at increasing the life options of disadvantaged young people through, for example, role models and mentoring, community service projects, job training, and activities aimed at reducing risky behaviors. Such interventions are expected indirectly to reduce levels of unintended teenage pregnancy and childbearing and sexually transmitted infections, in the belief that teenagers who are more positive about their futures are less likely to participate in risk-taking behaviors, including risky sexual practices.
Other policies or programs implemented with the hope of reducing unprotected teenage sexual behavior include: (1) comprehensive school-based sexuality education curricula that include discussion of abstinence, but also include information about contraceptive methods and services; (2) programs that address the social pressures faced by teens to have sex and that provide modeling and practice of communication, negotiation, and refusal skills; (3) condom availability programs in schools; and (4) multicomponent programs that include community-wide activities, such as media involvement, social marketing, and links between school-based activities and contraceptive service providers.20
Evaluations of a variety of programs and approaches aimed at affecting teenage sexual and reproductive behavior have shown that some programs have had a positive effect on the behavior of youth. In addition, results of multiple studies indicate that the provision of contraceptive information and access does not encourage youth to become sexually active at younger ages. Reviews of the evaluation research suggest that greater success may be achieved through integrated approaches that address both the antecedents of sexual risk-taking (e.g. poverty, violence, social disorganization), as well as provide young people with the information, skills, and resources to make responsible decisions about sexual behavior and the avoidance of unintended outcomes.21
REFERENCES
Guttmacher Institute, 2008, tabulations of the 2002 National Survey of Family Growth (Cycle VI) |
|
Chandra A, Martinez GM, Mosher WD et al: Fertility, family planning, and reproductive health of U.S. women: data from the 2002 National Survey of Family Growth. Vital Health Stat 23. 2005 Dec;(25):1-160. |
|
Forrest JD: Timing of reproductive life stages. Obstet Gynecol. 1993 Jul;82(1):105-11. |
|
Frost JJ: Trends in US women's use of sexual and reproductive health care services, Am J Public Health. 2008 Oct;98(10):1814-7. Epub 2008 Aug 13. |
|
Scholle SH, Chang JC, Harman J et al: Trends in women's health services by type of physician seen: data from the 1985 Womens Health Issues. 2002 Jul-Aug;12(4):165-77. |
|
Frost JJ. Using the NSFG to examine the scope and source of contraceptive and preventative reproductive health services obtained by US women, 1995-2002. Paper presented at: The 2006 Research Conference on the National Survey of Family Growth; October 2006; Hyattsville, MD. |
|
Frost JJ, Frohwirth L, Purcell A: The availability and use of publicly funded family planning clinics: U.S. trends, Perspect Sex Reprod Health. 2004 Sep-Oct;36(5):206-15. |
|
The Alan Guttmacher Institute: Uneven & Unequal: Insurance Coverage and Reproductive Health Services. New York, The Alan Guttmacher Institute, 1994 |
|
Ortho-McNeil: Tabulations from the 1996 Ortho Birth Control Study, Ortho-McNeil, 1997 |
|
Mosher WD: Contraceptive practice in the United States, 1982-1988. Fam Plann Perspect 22: 198, 1990 |
|
Guttmacher Institute, 2008, tabulations of the 1982, 1995 and 2002 National Surveys of Family Growth. |
|
Frost JJ, Darroch JE, Remez L: Improving contraceptive use in the United States. Issues Brief (Alan Guttmacher Inst). 2008;(1):1-8. |
|
Frost JJ, Singh S, Finer LB: U.S. women's one-year contraceptive use patterns, 2004. Perspect Sex Reprod Health. 2007 Mar;39(1):48-55. |
|
Frost JJ, Singh S, Finer LB: Factors associated with contraceptive use and nonuse, United States, 2004. Perspect Sex Reprod Health. 2007 Jun;39(2):90-9. |
|
Forrest JD, Frost JJ: The family planning attitudes and experiences of low-income women. Fam Plann Perspect 28: 246, 1996 |
|
Finer LB, Henshaw SK: Disparities in rates of unintended pregnancy in the United States, 1994 and 2001. Perspect Sex Reprod Health. 2006 Jun;38(2):90-6. |
|
Henshaw SK: Unintended pregnancy in the United States. Fam Plann Perspect 30: 24, 1998 |
|
Jones R et al., Repeat abortion in the United States, Occasional Report, New York: Guttmacher Institute, 2006, no. 29. |
|
Singh S, Darroch JD: Adolescent pregnancy and childbearing: Levels and trends in developed countries. Fam Plann Perspect 32: 14, 2000 |
|
The Alan Guttmacher Institute: Sex and America's Teenagers. New York, The Alan Guttmacher Institute, 1994 |
|
Kirby D: Emerging answers: Research findings on programs to reduce teen pregnancy. Washington, DC, National Campaign to Prevent Teen Pregnancy, 2001 |